

I am Dr. Chou, President and Director of Sincere Dermatology Clinic. With 15 years of experience as a dermatologist, I specialize in trichology and addressing various skin concerns. I have compassionately cared for patients with scalp conditions like psoriasis and seborrheic dermatitis, providing effective management strategies to alleviate symptoms and improve their well-being.
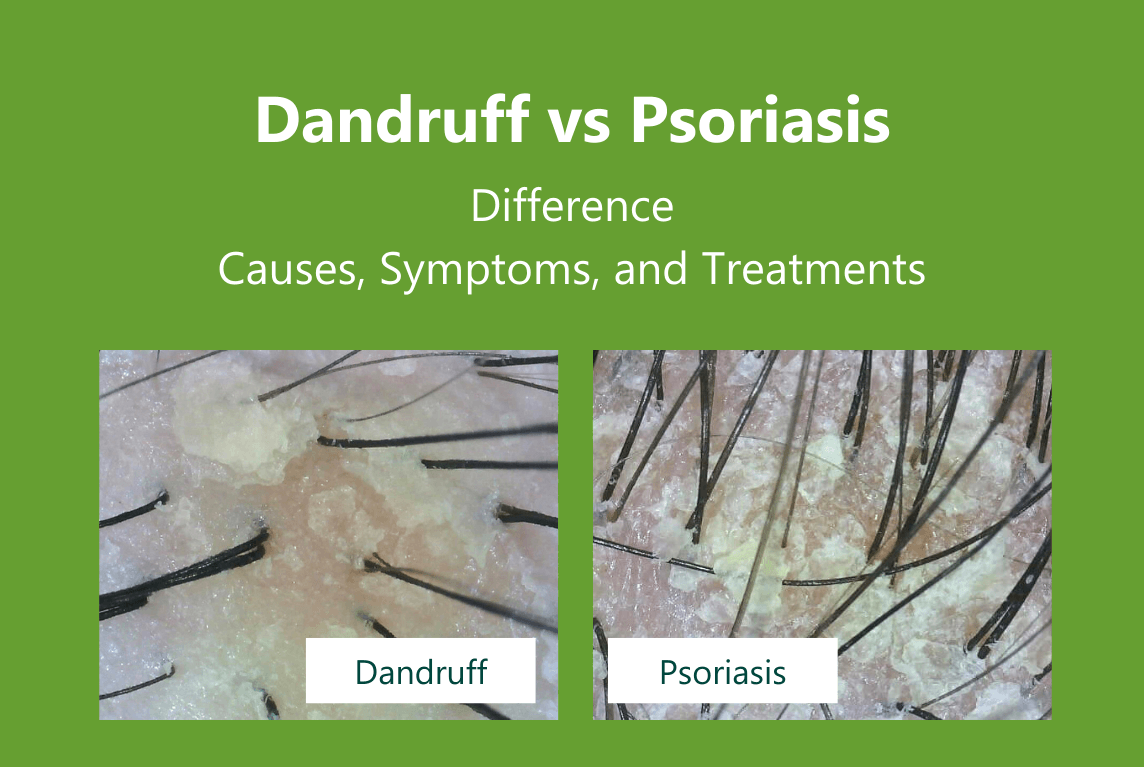
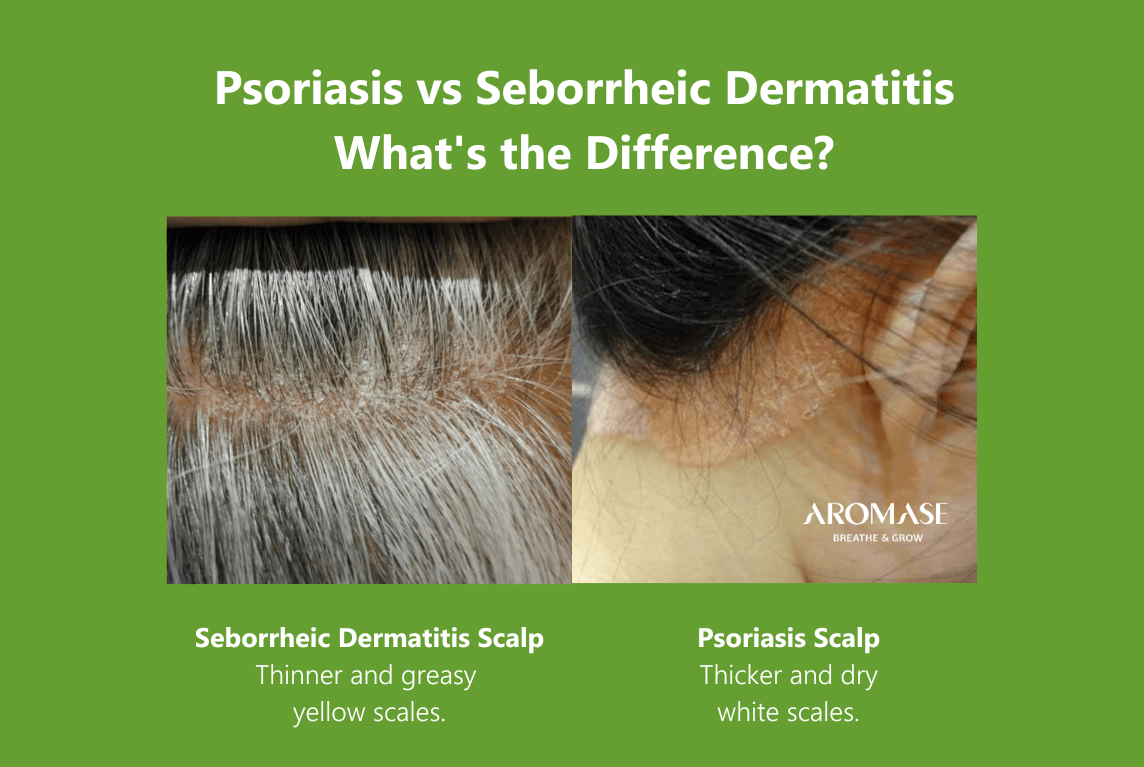
How to distinguish scalp psoriasis from seborrheic dermatitis?
Scalp seborrheic dermatitis and psoriasis can be difficult to distinguish clinically. If the diagnosis is difficult, a “sebopsoriasis” diagnosis may be made temporarily, with dermatologists waiting to see if more typical lesions develop on other sites later on.
| Seborrheic Dermatitis | Psoriasis | |
|---|---|---|
| Thickness of the scales | Thinner | Thicker |
| Scales appearance | Greasy | Dry |
| Range of lesions | Within the hairline | Beyond the hairline |
| Color | Yellow or white | Silvery white |
| Other lesion locations | Face (glabellar area, nasolabial folds), ears, anterior chest |
Everywhere of the skin, nails |
| Risk for arthritis | None | 3 folds |
| Dermoscopy The visual depiction of the specimen when observed under a microscope. |
Arborizing vessels |
Dotted
Globular Glomerular vessels |

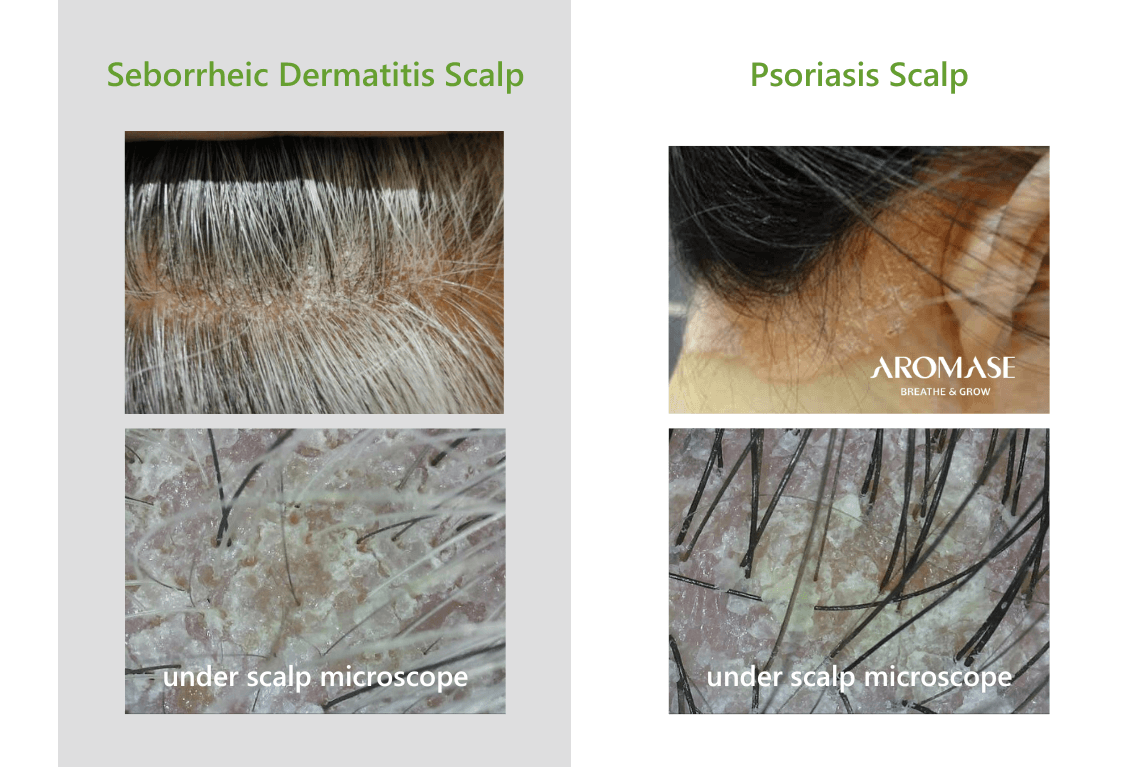
Under Microscope: What do the symptoms of Psoriasis & Seborrheic Dermatitis scalp look like?
How to diagnose psoriasis?
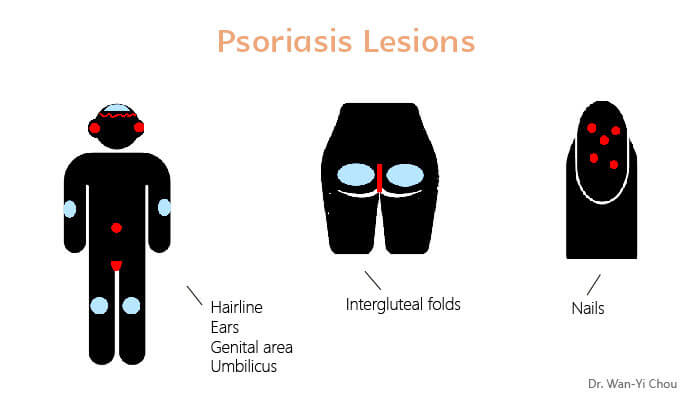
The detective spirit: Don’t forget to check the hairline, ears, genital area, umbilicus, intergluteal folds, and nails.
The job of a dermatologist is similar to that of a detective, requiring the use of challenging diagnostic methods.
- Medical history
- Clinical findings
Clinically, differential diagnosis between psoriasis and many diseases such as seborrheic dermatitis or chronic dermatitis is required. However, psoriasis is much like a clumsy robber who leaves many clues waiting for the dermatologists to uncover.
Plaque-type psoriasis typically manifests in specific areas of the body. The scalp, extremities (which are susceptible to injury or friction), and lower back are the primary distribution sites (marked in blue). However, if no psoriatic lesions are observed in these areas, we can look for signs of psoriasis in the hairline, ears, genital area, umbilicus, intergluteal folds, and nails (indicated by a red color).
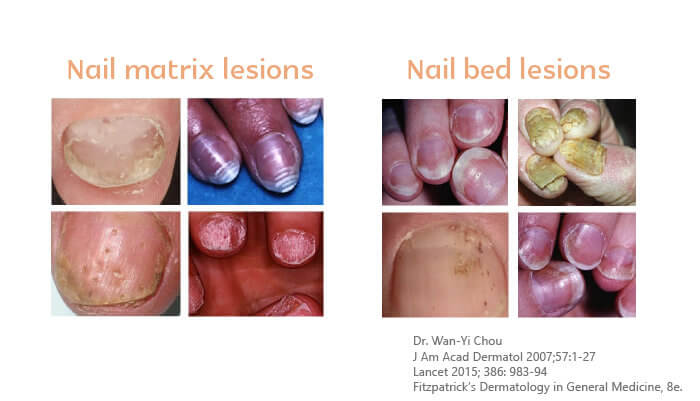
Nail manifestations
Nail manifestations are subdivided into two categories:
- Nail matrix lesions: red spots in lunula, leukonychia, pitting, or nail plate crumbing
- Nail bed lesions : onycholysis, subungual hyperkeratosis, splinter hemorrhages, or oil drops.
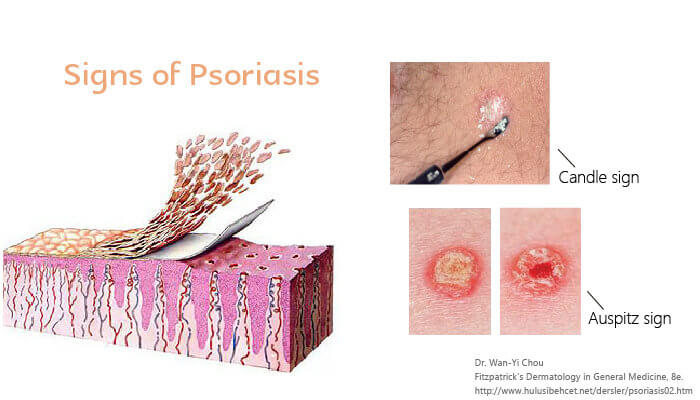
Pathologic examination shows the incomplete keratinization (parakeratosis) of the stratum corneum, when we use the wooden end of a swab to scrape a lesion, it is like scraping a candle where silvery white dander continues to fall off (candle sign). Additionally, due to the dilated capillaries of the papillary dermis and the thin epidermis layer above it, as we continue to scrape harder, we will see punctate bleeding spots (Auspitz signs). This is why when patients suspected of having psoriasis arrive in my clinic, I will take a cotton swab for scrapping.
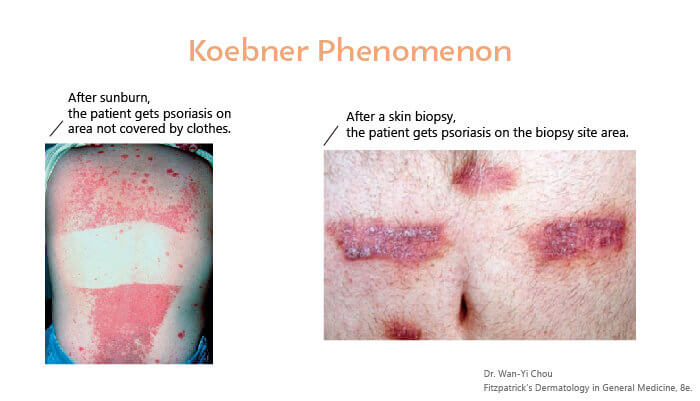
Another special part about psoriasis is that it is found on a skin injury site. When it is difficult to determine clinically, the dermatologist’s ultimate secret weapon is skin biopsy.
The picture on the left shows a sunburned psoriasis patient with visible psoriasis lesions on uncovered skin, while the picture on the right shows a patient with a dry sore at the site of a skin biopsy.
It’s a journey, not a destination.
While there is no definitive cure for psoriasis or dermatitis, many of my patients have found effective ways to alleviate symptoms and manage their condition. If you are unsure whether you are experiencing psoriasis or seborrheic dermatitis, it is crucial to seek professional medical advice for accurate diagnosis and appropriate treatment.
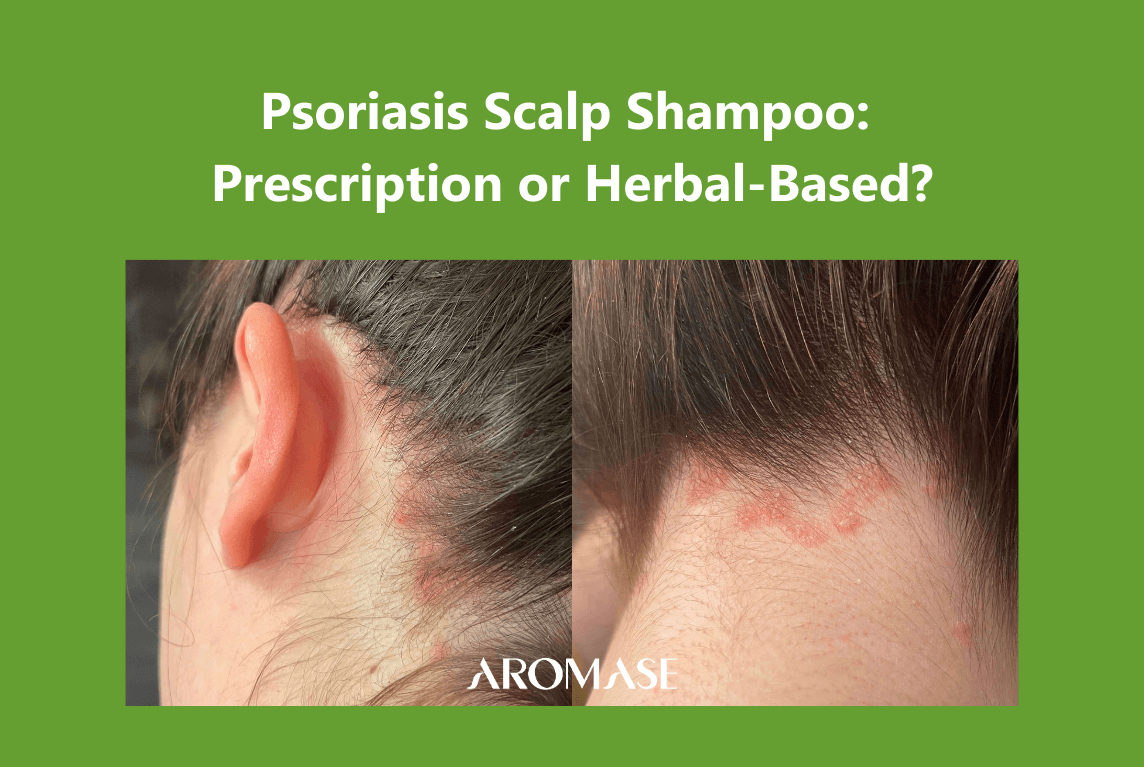
3 Steps Treatment for Psoriasis scalp
Calm your psoriasis scalp: Psoriasis Scalp Care 3 Steps Solution
What’s included: scalp deep cleanser + daily shampoo+ scalp tonic

3 Steps Treatment for Dermatitis scalp
Calm your psoriasis scalp: Oily Dandruff 3 Steps Solution ( Ideal for Dermatitis)
What’s included: scalp deep cleanser + daily shampoo+ herbal cooling scalp spray

References:
- J Am Acad Dermatol 2008; 58(5):826-850.
- Ann Rheum Dis 2005; 64:18-23
- Journal of Dermatological Science. 2011; 63:40–46
- Fitzpatrick’s Dermatology in General Medicine, 8e.
- British Journal of Dermatology 2007;156, pp258–262
- https://www.dermnetnz.org/topics/guidelines-for-the-treatment-of-psoriasis/
- Lancet 2015; 386: 983–94
- Rheum Dis 2005;64(Suppl II):ii30–ii36
- Golpour Dermatology Research and Practice Volume 2012, Article ID 381905,
- Dermatology 2007;215:17–27
- Arch Dermatol Res (2006) 298:321–328
- Br J Dermatol. 2010 Sep;163(3):586-92
- Br J Dermatol. 2007 Feb;156(2):258-62.
- British Association of Dermatologists 2011 164, pp652–656
- J Am Acad Dermatol 2007;57:1-27.
- psoriasis forum, SPRING 2012 Vol. 18, No. 1